
Historically, LDL cholesterol (LDL-C) has occupied the spotlight in atherosclerotic cardiovascular disease (ASCVD), as it is a causal factor in arterial blockages.
However, LDL-C is only one component of a multivariable disease.
Only recently has a cholesterol lipoprotein that is potentially 5-6 times more atherogenic than LDL-C been brought to the forefront.
It's called lipoprotein(a) [Lp(a)] — pronounced: "L-P-little-a."
It's the most common inherited cardiovascular risk factor in the world, affecting an estimated 1.5 billion people.
It's roughly 80-90% genetically determined. And until very recently, most patients had never heard of it — because most doctors weren't testing for it.
The National Lipid Association update, released in 2024, now recommends measuring Lp(a) in every adult at least once.
There's a good reason for that shift, and in today's newsletter, we will unpack what you need to know about Lp(a), the risk associated with your Lp(a) levels, what to do about it, and the medications on the horizon.
What is Lp(a) and What Makes it Dangerous?
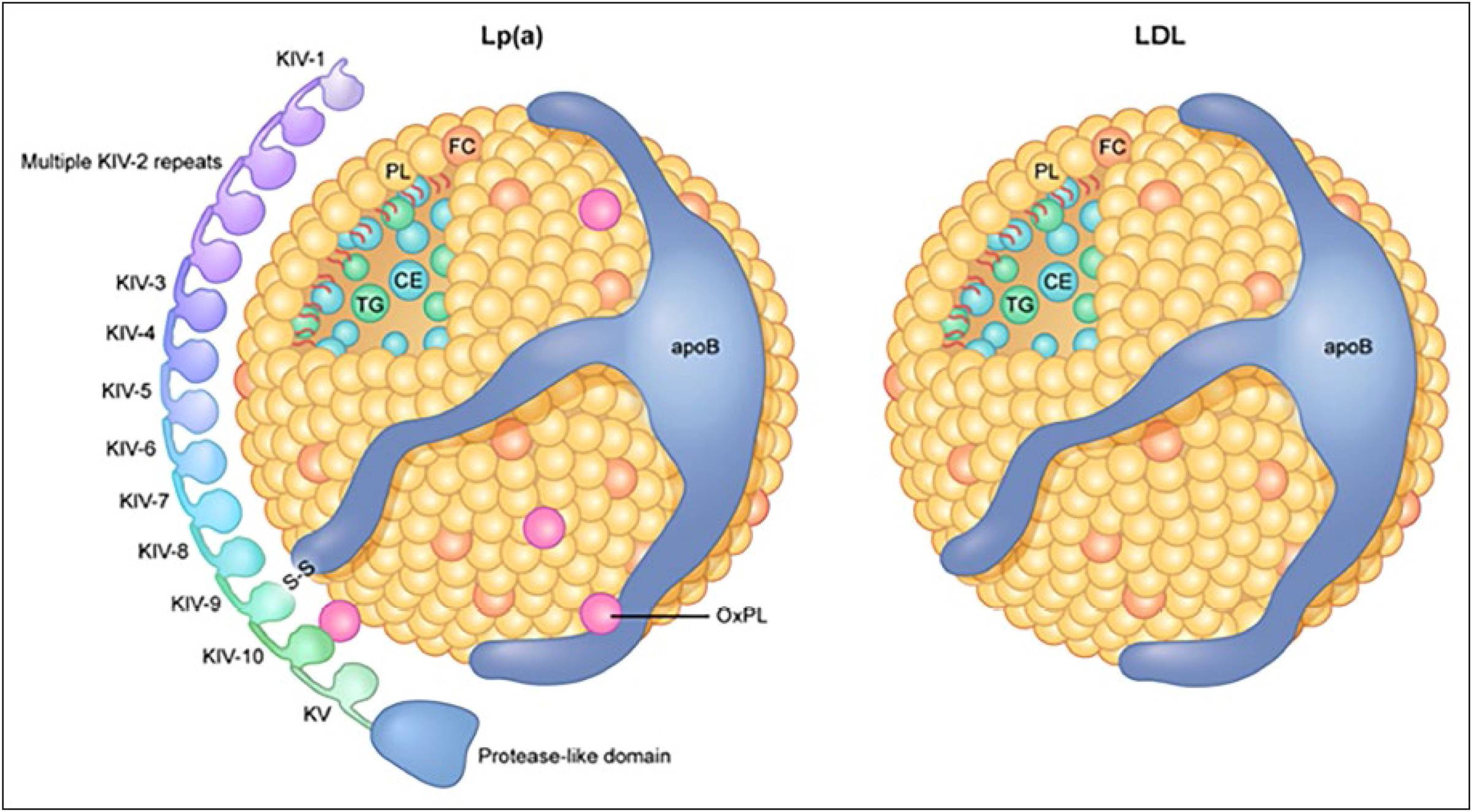
Picture an LDL particle.
Now imagine taking that LDL particle, adding a protein tail — a looped protein tail called apolipoprotein(a), or apo(a).
That's Lp(a). It's an LDL particle wearing an extra tail.
That extra tail changes everything.
First, the genetics. Your Lp(a) level is set almost entirely by the LPA gene you inherited from your parents.
Unlike LDL, it doesn't meaningfully respond to lifestyle choices.
You can run marathons, eat perfectly, and sleep great — and if you inherited a high-producing LPA gene, your Lp(a) will be elevated.
Now, Lp(a) doesn't cause symptoms, and it's not included on a standard lipid panel.
A patient can have a phenomenal cholesterol report from their primary care doctor and still be carrying an Lp(a) level four or five times the threshold for high risk.
What makes Lp(a) so bad?
This part surprises people, including many physicians.
On a per-particle basis, Lp(a) appears to be roughly six times more atherogenic than LDL.
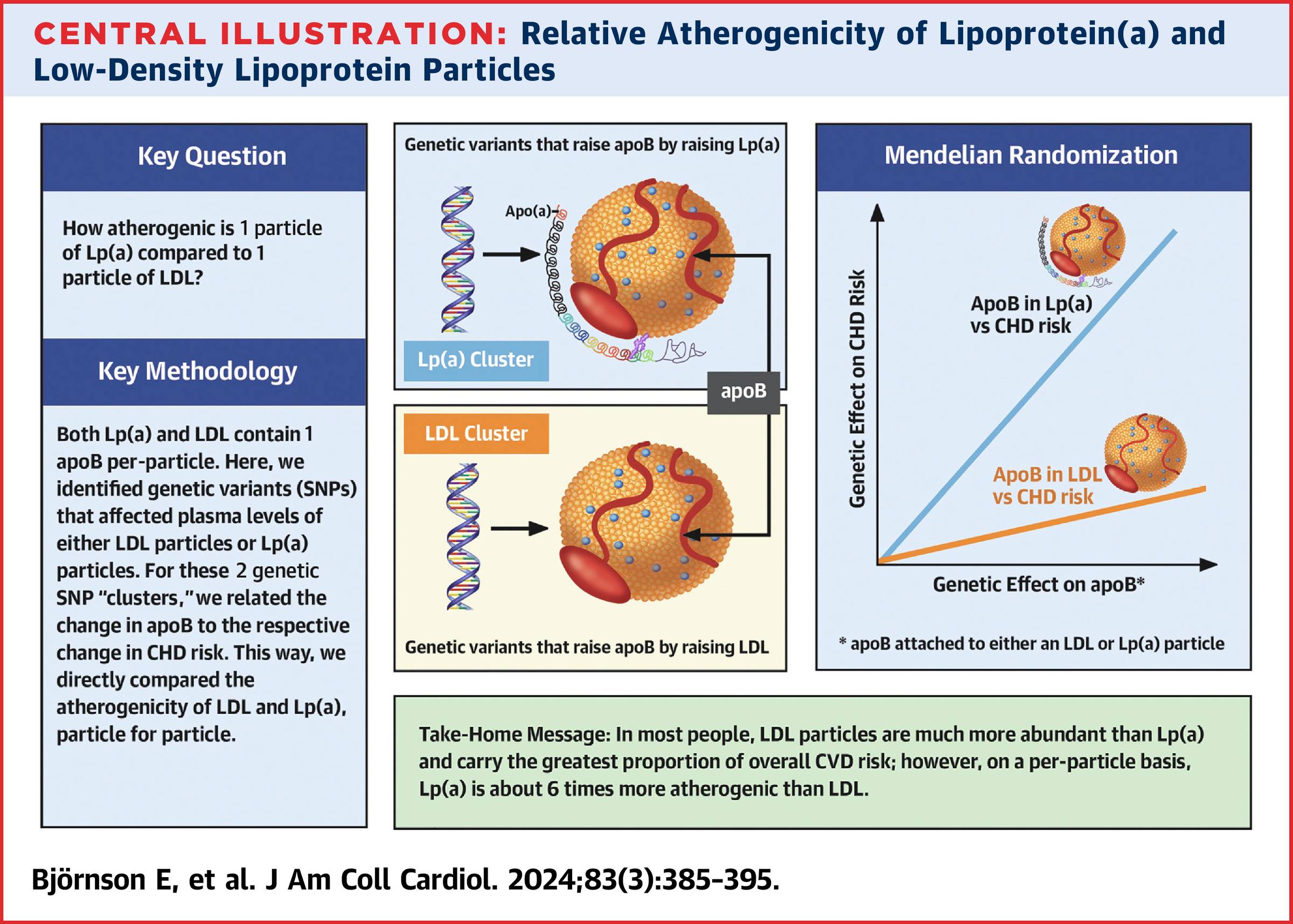
That estimate comes from a 2024 JACC analysis by Björnson and colleagues, which used a Mendelian randomization approach on UK Biobank data to compare the two particles head-to-head.
Particle for particle, Lp(a) drives more disease.
Why?
Three mechanisms at play:
- It does everything LDL does. Lp(a) crosses into the artery wall, gets retained by proteoglycans, and contributes to plaque just like LDL. That alone makes it atherogenic. But it doesn't stop there.
- It carries the inflammatory payload. Lp(a) is a major carrier of oxidized phospholipids in human plasma. Oxidized phospholipids are biologically active signaling molecules — they recruit monocytes into the artery wall, switch on inflammatory cytokines, and accelerate plaque growth. Most circulating oxidized phospholipids ride on Lp(a) specifically, which is in part why each Lp(a) particle punches so far above its weight class.
- It interferes with clotting. The apo(a) protein is structurally similar to plasminogen, the body's natural clot-buster. Lp(a) doesn't bust clots — it just looks like the thing that does. So it competes with plasminogen at the site of injury, potentially slowing the body's natural process of breaking down and dissolving blood clots.
The net effect: Lp(a) may make the clots that form harder to break down.
Triple threat: atherogenic, inflammatory, and pro-thrombotic.
"If It's Genetic and There's No Cure, Why Test?"
This is a valid question we are often asked.
Why test Lp(a) if levels are inherited, unchangeable, and only cause patient anxiety?
This thought process initially halted testing; however, the landscape has shifted.
Understanding your Lp(a) levels gives you a better picture of your overall risk profile.
Cardiovascular risk isn't one number. It's a stack — ApoB / LDL-C, blood pressure, insulin resistance, inflammation, smoking, and family history, to name a few.
Lp(a) sits on top of that stack as a damage multiplier.
Though lifestyle and medical intervention can not directly lower your Lp(a), they are levers to pull to decrease your overall risk.
If your Lp(a) is elevated, it's another reason to double down on lifestyle and potentially medical intervention to control the surrounding risk factors.
Understanding Your Lp(a) Result
A note on Lp(a) units.
Lp(a) can be reported in two different units:
- mg/dL (measuring mass)
- nmol/L (measuring particle number).
Particle number is the preferred unit.
The conversion between the two is imperfect because Lp(a) particles vary in size, but as a rough guide, multiply mg/dL by ~2.5 to estimate nmol/L.
Using the 2024 NLA thresholds:
- Under 75 nmol/L (under ~30 mg/dL): Low risk. This is most of the general population.
- 75 to 125 nmol/L (30–50 mg/dL): Intermediate / "gray zone." Worth a repeat measurement to confirm, and worth tightening up other risk factors.
- 125 nmol/L and above (50 mg/dL and above): High risk. This represents roughly 20–25% of the population. Risk climbs continuously from here — the higher you go, the steeper the curve.
- Above 175–200 nmol/L: Very high risk. This is where the trial entry criteria for the emerging therapies are being set, and it correlates with risk levels comparable to having familial hypercholesterolemia.
A few caveats. Lp(a) varies somewhat by ancestry — levels are typically higher in individuals of African ancestry, and the risk thresholds may not translate identically across all populations.
Acute inflammation can transiently raise levels. And if your value falls in the 75–125 gray zone, a repeat measurement helps clarify.
The Lp(a) Medication Horizon
Traditional cholesterol therapy (Statins, ezetimibe, etc.) hasn't proven to meaningfully lower Lp(a) levels.
PCSK9 inhibitors do lower Lp(a), but the reduction is modest — approximately 20–30% — and considerably less than their effect on LDL-C (50–60%).
Four drugs are in advanced development, and most of them work by silencing the LPA gene itself — telling the liver to make less apo(a) in the first place.
Different mechanisms, different delivery, dramatically different from anything we've had before.
- Olpasiran (Amgen). An injection every three months. Lowers Lp(a) by more than 95%. Phase 3 outcomes expected in late 2026.
- Lepodisiran (Eli Lilly). Another long-acting injection. A single dose lowers Lp(a) by about 94% for six months. Enrolled in the largest of the ongoing trials — over 12,000 patients, including people without prior heart disease.
- Zerlasiran (Silence Therapeutics). Same general approach as olpasiran and lepodisiran. Over 90% reduction in Lp(a) with infrequent dosing.
- Muvalaplin (Eli Lilly). The wild card. This one is a daily pill — no injections. It works differently from the others by blocking Lp(a) from being assembled in the first place. Lowers Lp(a) by up to 86% in early trials. A pill that works this well would be a game-changer for access and adherence.
The critical question all of these trials are trying to answer: Does lowering Lp(a) actually prevent heart attacks and strokes?
We know elevated Lp(a) causes disease — we don't yet have proof that lowering it reverses the risk.
The first definitive answers are 12 to 24 months away.
Knowing Your Lp(a) Levels
As I mentioned, Lp(a) is not included in a standard lipid panel and is rarely included on routine annual labs.
If you are interested in knowing your Lp(a) levels, you can ask your primary care physician to order a test, or my family used Function to get our Lp(a) levels measured.
Function Health is an all-in-one health platform that starts with 160+ lab tests, covering your heart, hormones, liver, kidneys, thyroid, immune system, cancer signals, toxins, and key nutrients.
That’s about 5× more testing than standard primary care labs—bloodwork that would normally cost thousands of dollars out of pocket.
Scheduling is simple, with 2,000+ lab locations across the U.S., and most visits take around 15 minutes.
If you are interested in knowing your Lp(a) level, see if Function is a good fit for you.
Click here to sign up for Function Health for less than $1/day
Only the best,
Jeremy London, MD
P.S. Don't forget to follow my podcast for free on Spotify or Apple Podcasts
Related Articles




























































Subscribe for Free to Keep Reading
This content is free, but you must be subscribed to keep reading.