
One of the most requested topics to cover is cholesterol.
Over the past few years, there has been an emotional uproar about the effects of cholesterol and its role in heart disease.
Despite what you may see on social media, today's newsletter will take a deep dive into how cholesterol contributes to atherosclerotic cardiovascular disease (ASCVD).
As a heads-up, this newsletter will be more involved to give adequate context and attention to this polarizing topic.
I'm going to hold off on covering medical therapies such as statins, PCSK9 inhibitors, and ezetimibe in this edition and focus solely on cholesterol.
Let's dive in.
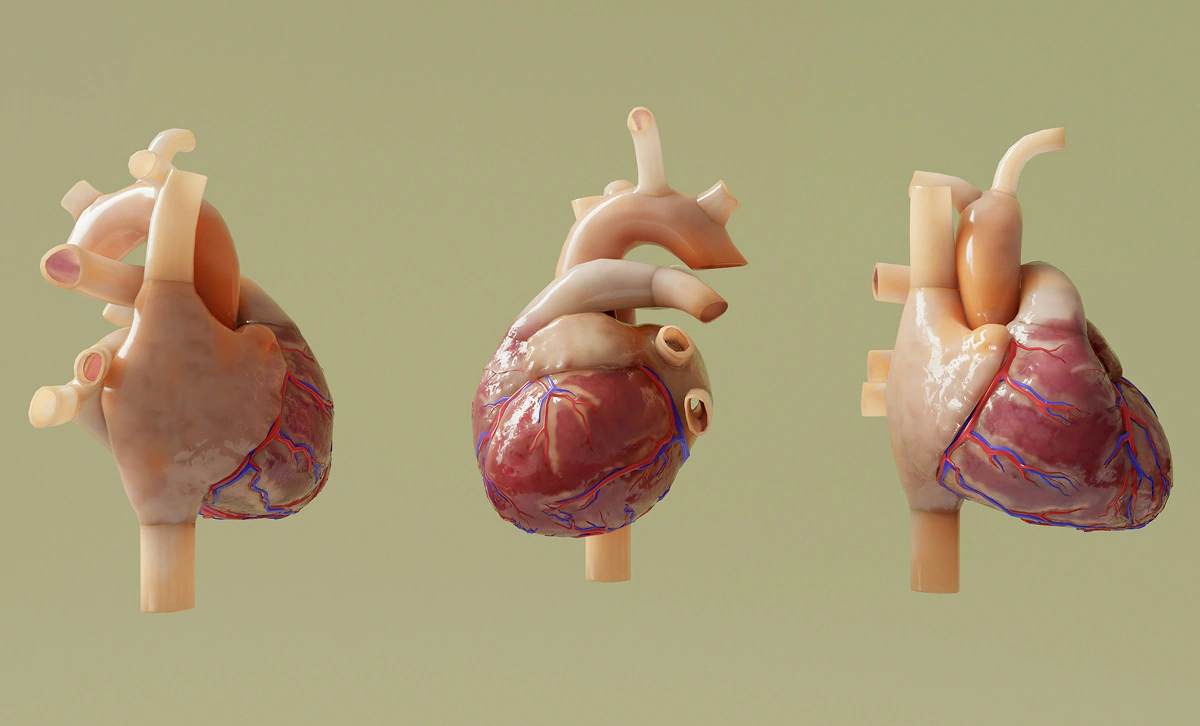
Cholesterol: The Basics & Foundation
To better understand cholesterol's role in heart disease, we need to start with the basics.
Surprisingly, cholesterol is absolutely essential for human survival.
Without cholesterol, you wouldn't be alive.
Cholesterol is fundamental to cell membrane structure, nerve pathway development, hormone synthesis, and vitamin D synthesis.
The next key component is how cholesterol is transported throughout your body.
Cholesterol is fat-like (lipophilic), and your blood is predominantly water; this makes transport difficult without a carrier.
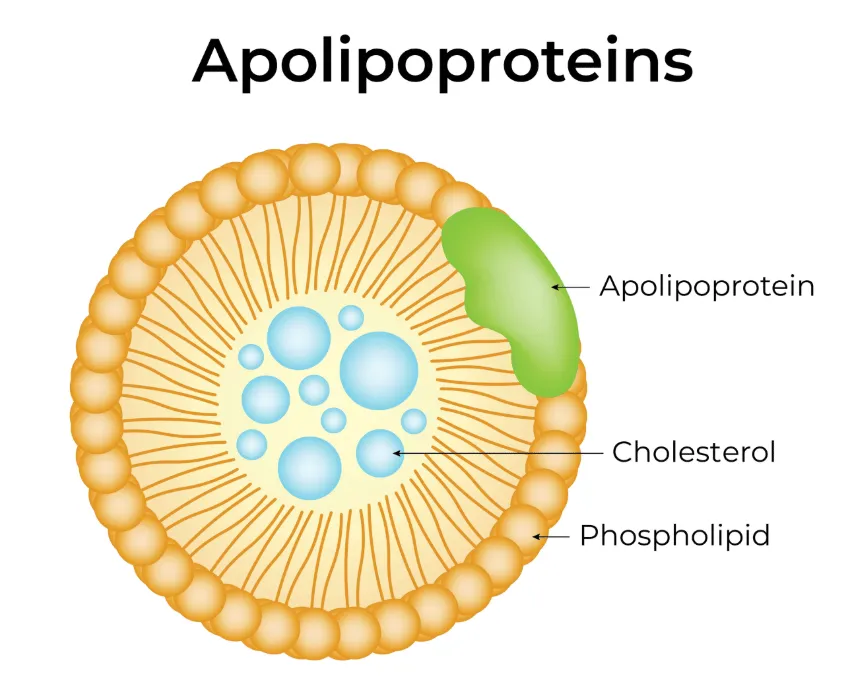
Introducing lipoproteins.
Cholesterol is packaged in water-soluble proteins to make it soluble. Think of lipoproteins as the cargo ships that can move cholesterol throughout your bloodstream.
Ironically, the lipoproteins solve the transport issue but introduce the next set of problems.
Apolipoprotein B (ApoB) particles can specifically bind to the endothelium of blood vessels and trigger the atherosclerosis cascade.
ApoB particles represent all the atherogenic cholesterol particles, including LDL-C, VLDL, IDL, and Lp(a).
Though cholesterol itself is essential, the more apolipoprotein B particles in the bloodstream, the higher the chances that the particles can slip through the endothelium and get trapped in the subendothelium.
This is the problem we are going to dig into today.
Does Cholesterol Cause Heart Disease?
Heart disease isn't the outcome of a singular variable.
There are multiple ingredients that can increase your risk profile of developing heart disease.
High levels of cholesterol, specifically apolipoprotein B particles, are a key factor.
As are chronic high blood pressure, high blood sugar, chronic stress, and obesity.
My point is that cholesterol isn't the sole defining factor in the puzzle.

Let's walk through how these lipoproteins can contribute to the atherosclerosis cascade process:
- ApoB particles in circulation penetrate the arterial wall and cross into the intima (inner lining of the artery).
- The particles become trapped and undergo chemical changes, such as oxidation or glycation. Now, these particles are foreign to the immune system, and the body's defense and repair processes begin.
- Immune cells are sent to the site of penetration and convert the lipids into foam cells. These foam cells progress into fatty streaks that can promote plaque progression. More susceptible to ApoB particles, more immune activity, increases the cycle.
- This can lead to two outcomes:
- A stable plaque that accumulates over time, which can lead to predictable symptoms.
- An unstable plaque that can rupture and activate clot formation, blocking the vessel, resulting in a heart attack or stroke.
Heart disease doesn't happen overnight.
Most of the time, ASCVD requires decades of cumulative exposure.
Conceptual:
(ApoB particle number) × (time) = Heart Disease Risk
Now that we have covered the basics of cholesterol, lipoproteins, and the atherosclerotic cascade, let's look at the data that support these concepts.
The Data: Impossible to Ignore
As we alluded to earlier, there is a wave of emotion around cholesterol on social media, but we need to ensure our decisions are based on data.
Does the equation above (Apob particle number) x (time) = Heart Disease Risk stand true in the data?
Since this disease progresses over a lifetime, the bad news is that actively running a randomized control trial for 50+ years would be extremely expensive and difficult to monitor.
Incredibly, nature designed this study for us. We are assigned genes at birth, and with the endless combinations and variations, we are effectively randomized into different groups.
How does this relate to our newsletter today?
Can we examine the risk difference between individuals with genetic predispositions to high vs. low lifetime ApoB exposure?
Some people are born with genes that naturally lower their cholesterol. Researchers can follow these people for decades and compare their risk of heart disease with that of the general population. Because genes are assigned randomly at birth, this acts like a “natural clinical trial.”
This is essentially what Mendelian Randomization studies accomplish.
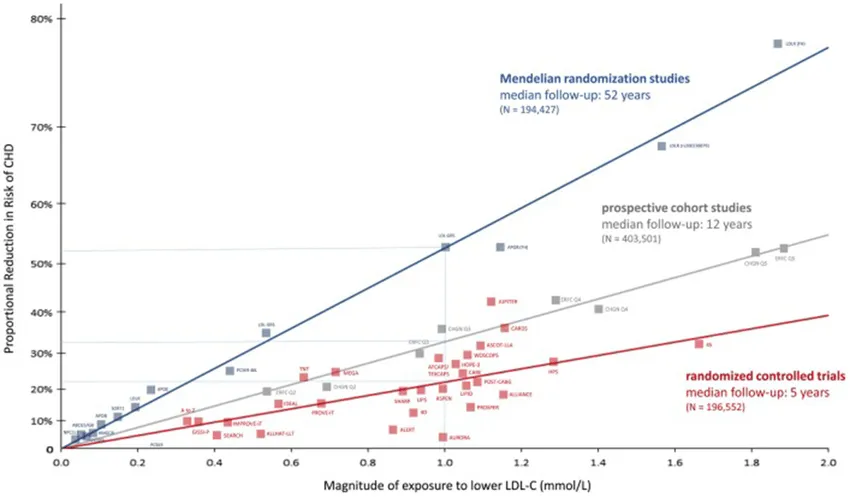
This chart plots the amount of LDL cholesterol lowered on the X-axis against the percent reduction in coronary heart disease (CHD) risk on the Y-axis.
In simple terms, it shows that greater LDL reduction is associated with greater heart-disease risk reduction—but the relationship isn’t the same across all types of studies.
The three lines highlight when LDL is lowered and for how long.
- Red represents randomized controlled trials (≈5 years of treatment)
- Gray represents prospective cohort studies (≈12 years),
- Blue represents Mendelian randomization studies in which LDL is lower from birth (≈approximately 50+ years).
For the same LDL reduction, lifetime exposure produces dramatically greater risk reduction—roughly double that seen in short-term trials.
The key takeaway is that time matters as much as magnitude: lowering LDL earlier and maintaining it longer has a far larger impact on preventing atherosclerosis than starting later, even if the cholesterol drop is identical.
Lowering LDL cholesterol works a lot like investing in the stock market. You can invest a large amount later in life and still see gains, but the real power comes from starting early and letting compounding do its work.
Mendelian randomization studies show that when LDL is lower from the very beginning, the benefits accumulate year after year, leading to a dramatically lower lifetime risk of heart disease.
Short-term LDL lowering still helps, just like late investing still grows your money, but it can’t match the impact of decades of steady compounding.
In cardiovascular health, as in investing, time in the system matters more than timing.
Due to the long nature of this newsletter, I have attached studies worth exploring:
- Effects of apolipoprotein B on lifespan and risks of major diseases, including type 2 diabetes: a mendelian randomisation analysis using outcomes in first-degree relatives
- Evaluating the relationship between circulating lipoprotein lipids and apolipoproteins with risk of coronary heart disease: A multivariable Mendelian randomisation analysis
- ApoB-containing lipoproteins: count, type, size, and risk of coronary artery disease
- Association of Triglyceride-Lowering LPL Variants and LDL-C–Lowering LDLR Variants With Risk of Coronary Heart Disease
Addressing Frequently Asked Questions & Concerns
"I saw someone live to 100 years old with super high LDL. This doesn't make sense!
Whenever we refer to risk factors, we are talking about a game of probability. Exposure to high concentrations of ApoB / LDL increases your risk of coronary heart disease, but there are no guarantees. Blockages may be present in non-lethal areas that don't result in a heart attack or stroke.
The false assumption is that they lived to 100 because of high LDL. There will almost always be exceptions to the rule, but when we look at data from millions of people, there is an increased risk with exposure to higher levels.
Would you rather bet your life on a few outliers or on the millions?
"People with 'normal' cholesterol levels still have heart attacks - How?
In most cases, 'normal' means average risk, not optimal.
This is considered significantly lower than the 'normal' levels suggested; plaque progression occurs with levels above this, and blockages can still occur.
"Why is ApoB a more accurate indicator than LDL-C?
Every atherogenic lipoprotein that can enter the arterial wall carries one ApoB molecule: LDL, VLDL, IDL, and Lp(a).
More particles = more opportunities to damage the artery wall.
LDL-C measures how much cholesterol mass is inside LDL particles — not how many particles exist.
Discordance can occur when LDL-C is normal, but ApoB is elevated.
"Why does pharmaceutical lowering therapy not prevent all heart attacks?
Lipid-lowering therapy doesn't fully eliminate the chance of heart attacks, but it does two things at once: it slows or halts new plaque formation and stabilizes existing plaques, making rupture much less likely.
The fewer ApoB particles circulating over time, the fewer opportunities there are for arterial complications.
However, the relationship is dose-dependent and time-dependent, so the risk depends on when the treatment was implemented.
Finally, there are additional causes why heart attacks occur besides blockages from lipoproteins.
My Final Thoughts
If you are still reading this newsletter, I appreciate your interest and your attention.
The takeaway from this article is that cholesterol is essential to our health, but the number of ApoB particles matters for heart disease.
The popular myth that cholesterol doesn't matter is dangerous, and your levels should not be ignored.
Cholesterol (specifically lipoproteins) isn't the only factor, but it's a key one.
Lifestyle modifications and medical therapy (consult your qualified healthcare professional to determine whether you are a candidate) should be considered to mitigate risk.
Be proactive and stack the deck in your favor.
I want to hear your thoughts and feedback:
Was this newsletter helpful? What questions do you still have after reading this article? Thoughts you want to share?
Reply directly to this email (Yes, I read all responses).
What Makes Rho Different
Rho Nutrition because they bring something different to your fridge.
Rho offers third-party-tested liposomal delivery products. Why does this matter? Most pills and powders lose a significant amount of the active ingredient during digestion.
Rho encapsulates each nutrient (creatine, glutathione, NAD+, curcumin, collagen, etc.) within a tiny liposome that survives the gut and ferries the compound intact into the bloodstream.
Liposomal delivery helps ensure that the vitamins and supplements you purchase are getting absorbed and not lost during digestion.
My personal morning Rho stack is their liposomal creatine, glutathione, DIM+, and NAD+, and before bed, I take their liposomal magnesium.
The founders, Ryan and George, firmly believe you will feel the Rho difference, but if you're not satisfied, they offer a 60-day money-back guarantee.
Click here to save 20% and add Rho to your daily routine
Only the best,
Jeremy London, MD
P.S. Don't forget to follow my podcast for free on Spotify or Apple Podcasts
Related Articles






































































Subscribe for Free to Keep Reading
This content is free, but you must be subscribed to keep reading.